
Revista Iberoamericana de Neuropsicología
Vol. 2, No. 1: 55-67, enero-junio 2019.
Executive functioning performance of bilingual and monolingual children with a traumatic brain injury
Isabel Gonzalez, Psy.D., LMHC, LMFT1, Miriam J. Rodriguez, Ph.D2, Isaac Tourgeman, Ph.D3, Suzan Tanner Woodward, Ph.D.4
1,2,3 Albizu University, Miami, Florida
4 Jackson Memorial Hospital, Miami, Florida. Director, Pediatric Neuropsychology Program (Retired)
[su_row][su_column size=”1/2″][su_button url=”https://neuropsychologylearning.com/wp-content/uploads/pdf/pdf-revista-vol2/RevistaNeuro3Binder24Ene19-58-70.pdf” target=”blank” style=”flat” background=”#F38546″ color=”#ffffff” size=”6″ radius=”0″ icon=”icon: arrow-down” icon_color=”#ffffff” text_shadow=”0px 0px 0px #ffffff”]ARTÍCULO[/su_button][/su_column] [su_column size=”1/2″][su_button url=”https://neuropsychologylearning.com/wp-content/uploads/pdf/pdf-revista-vol2/RevistaNeuro3Binder24Ene19.pdf” target=”blank” style=”flat” background=”#F38546″ color=”#ffffff” size=”6″ radius=”0″ icon=”icon: arrow-down” icon_color=”#ffffff” text_shadow=”0px 0px 0px #ffffff”]REVISTA VOL2-N1[/su_button][/su_column] [/su_row]

Executive functioning performance of bilingual and monolingual children with a traumatic brain injury
Objective: The main purpose of this research study was to assess the difference between bilingual speakers and monolingual children who have sustained a TBI and their performance on a measure of executive functioning. It is hypothesized that 1) age would be a significant contributor to performance on executive functioning tasks, 2) neurocognitive performance on measures of executive functioning will be lower for the TBI group as compared to the control group, and 3) neurocognitive performance on measures of executive functioning will be lower for monolingual as compared to bilingual peers. Method: The total sample consisted of 48 children. Each subject was administered the D-KEFS (1), as part of a larger neuropsychological battery. The hypotheses were tested using appropriate independent-samples tests to determine whether statistically significant differences existed in executive functioning performance between groups. Furthermore, age was treated as a continuous variable, and was tested for normality. Results: Significant difference were found between the TBI and Control groups for CW4 [t(36)=3.121, p =.003], TMT 2 [t(40)=3.175, p =.003], and TMT 3 [t(40)=3.259, p =.002]. When comparing the performance of monolinguals and bilinguals, statistically significant results where found for the control group (Mann Whitney U = 11, n1=10, n2=6, p=0.044), but not for the TBI group (Mann Whitney U = 54, n1=11, n2=10, p=0.968). Age was not found to be be a significant contributor to performance. Conclusion: Bilinguals without a TBI demonstrated a significant advantage in a verbal task of inhibition and switching. Overall results demonstrate children’s higher order functioning abilities are significantly impacted by a TBI. Interestingly, bilingual children seem to be at an increased risk of executive functioning impairments after a TBI. This could be the result of a newly acquired skill and the damage to a less mature region of the brain.
Keywords: Executive Functioning, Brain Injury, Bilingualism, and Children
Acquired brain injuries occurring after 3 months of age can be divided into traumatic brain injury (TBI), caused by trauma to the brain, or non-traumatic brain injury (NTBI), due to medical pathologies (stroke, hypoxia, tumor) (2). TBI results from acute external forces to the skull resulting in extensive lesions to the neural tissue and diffuse axonal damage (3). TBI results in neurocognitive deficits, affecting attention, motor performance, executive functioning, visuospatial abilities, auditory functioning, memory, language, emotional regulation, and sleep functions (3, 4, 5, 6). Multiple studies have demonstrated that the damaged brain may never return to its previous trajectory of development (7).
Although TBI is devastating at any point in the human development, research shows that young brains might be more vulnerable to slower recover and more severe, diffuse, and enduring deficits (8, 3, 5). Sadly, there is a high incidence of TBIs during childhood and early adulthood, time frames of rapid brain development (5, 7). According to the Center for Disease Control and Prevention (2016), children younger than 4 years of age have the highest rates (2193.8 per 100,000) of any age group, typically with almost twice the rate of those in the next highest age group (15–24 year-olds). Thousands of neural cells and synaptic connections are formed during brain development. Longitudinal analyses have shown that after a brain injury, late maturing regions of the frontal and temporal areas, fail to undergo expected cortical thinning producing long-standing cognitive impairment (7). Brain injury has the potential to affect subsequent development and prevents the brain from returning to its pre-injury baseline (7).
Interestingly, minorities in the United States of America seem to be at a greater risk of suffering a brain injury, as well as having worse predicted recovery outcome related to independent living, engagement in leisure activities, and return to work or school (9). Most of these minorities are bilingual. The U.S. Department of Education (2013) established that about 4.65 million individuals in the United States of America are identified as bilinguals. Bilingualism is defined as the constant use of two (or more) languages (10). Bilingual proficiency varies across the Hispanic population in the United States of America and it depends on many variables, such as the language exposure at school, language spoken at home, years of residence in countries with majority and minority languages, language deficits, and socioeconomic status (SES) (11).
Calabria et al., (12) suggested that bilinguals utilize a complex neural network involved in the use of more than one language. According to this hypothesis, each neural area is in charge of a specific cognitive function. Research also found that in bilinguals who sustained a brain injury, the level of activation and inhibition of both languages was significantly impaired (12). Tavano, et al (5) proposed that executive functions appeared as a characterizing cognitive sequel after brain injury. Banich (13) described executive functioning as action planning towards a goal, flexibility, sequencing, fluency, switching, inhibition, concept formation, estimation, prediction, and maintaining attentional sets. Executive control and inhibition develops during early adulthood and declines during aging. Such cognitive functions are responsible for the management of more than one language and in the language processing of bilinguals (14, 15, 16, 17, 18, 19).
Recent studies have demonstrated that cognitive reserve serves as an important moderator in the correlation between brain damage and clinical performance (20). Extensive research suggests that bilingualism acts as an important protective factor (cognitive reserve), delaying the manifestation of the symptoms of Alzheimer’s disease (15, 16, 20, 21, 22). According to this, the increased requirement of managing two languages seems to modify the clinical effects of brain damage (20). However, research has focused on two main issues, neurodegenerative diseases and bilingual aphasia. Up until now, only a small number of available studies have looked at the possible effects of bilingualism in children after sustaining a TBI. Given the high incidence of pediatric TBI, it is imperative to assess possible protective factors.
The main purpose of the current research study was to evaluate the difference between bilingual speakers and monolingual children who have sustained a TBI and their performance on measures of executive functioning. These results could be used to evaluate expected outcomes after brain injury and add information to the literature in an attempt to provide children with appropriate measures and remediation after a TBI.
Based on the available scientific data presented above, the current study proposes three hypotheses:
- It is hypothesized that age would be a contributor to performance on executive functioning tasks among the TBI and control groups.
- It was hypothesized that neurocognitive performance on measures of executive functioning would be lower for the TBI group as compared to the control group.
- It was hypothesized that neurocognitive performance on measures of executive functioning would be lower for monolinguals as compared to bilingual peers.
Archival data consisted of comprehensive neuropsychological testing completed at Jackson Memorial Hospital Pediatric Neuropsychology Outpatient Clinic. Data collection also included demographic information such as age, gender, grade level, educational status, ethnicity, family demographics, and dominant language, as well as related medical condition and diagnosis.
Participants
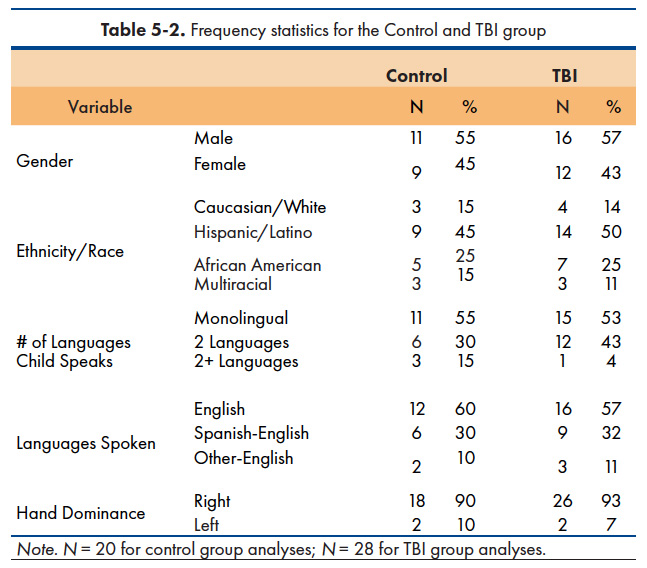
The total sample consisted of 48 children with a mean age of 14 (SD = 2.1) and ranged from 8 to 17 years old. Of those subjects, 56% was male and 44% was female. The range of education (in years) was 3 to 12 years. The sample’s ethnicity consisted of Hispanic/Latino (49%), African American/Black (25%), Caucasian/White (14%), and Multiracial (12%). The children each spoke between 1 and 4 languages, with most speaking only 1 language. 26 (54%) spoke only 1 language, 18 (37%) spoke 2 languages, and 4 subjects (9%) spoke more than 2 languages. Of all 48 individuals in the sample, 46 (96%) were tested in the English language. The last two individuals were tested with English and Spanish measures. A list of variables can be found in Table 5-2.
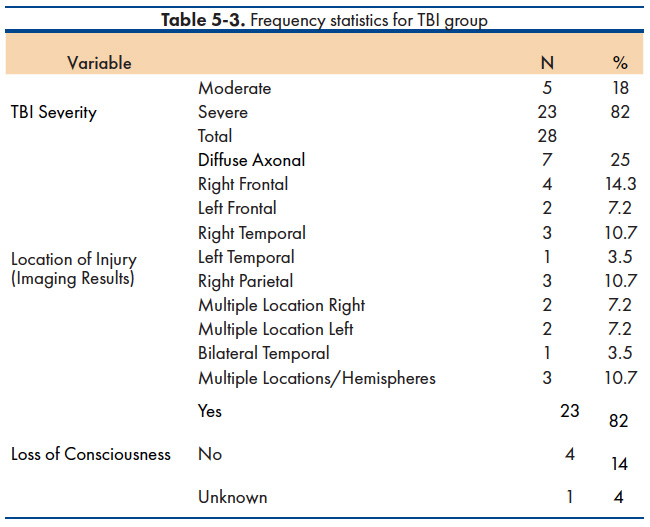
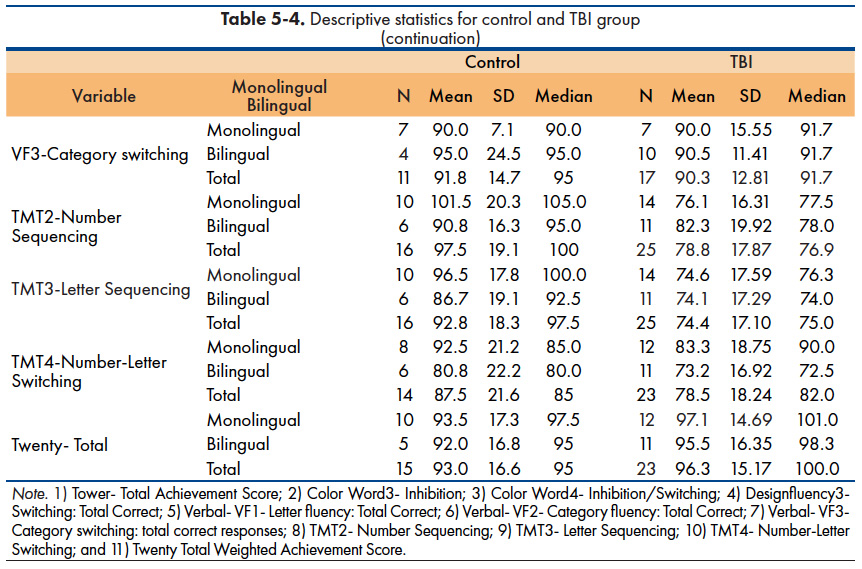
The data consisted of neuropsychological and intellectual measures from 2004 to 2017. Twenty subjects were included in the control group and met the following criteria: 1) medically healthy individuals with no previous history of TBI; 2) subjects who were identified as monolingual English speaker or bilingual speaker; and 3) subjects who had completed the D-KEFS and BRIEF measures. Exclusion criteria was based on history of a TBI and diagnosis including Cognitive Disorder NOS, Attention Deficit Hyperactivity Disorder (ADHD), and Anxiety and Related Disorders. Twenty-eight participants were included in the TBI group and met the following criteria: 1) subjects with confirmed moderate to severe TBI; 2) subjects who were identified as monolingual English speaker or bilingual speaker; and 3) subjects who had completed the D-KEFS measure. Due to the variability in presentation, not all subjects completed every subtest of the D-KEFS, and for this reason, some participants have missing scores for certain subtests (Table 5-3). Comorbid psychological or medical conditions were included to allow for greater generalization of this research project (Table 5-4).
Materials
A commonly used measure of executive functions was analyzed in the current study: the Delis-Kaplan Executive Function System (D-KEFS) The D-KEFS (Delis, Kaplan, & Kramer, 2001) is a set of measures that was designed to be used by well-trained clinicians in the comprehensive assessment of verbal and nonverbal executive functions, in both children and adults. The D-KEFS is composed of nine tests that assess a wide spectrum of verbal and nonverbal higher-order cognitive functioning. Each test was designed to be a stand-alone instrument that can be administered separately or together with other D-KEFS tests. For the purpose of this study, only the following tests would be analyzed: Trail Making Test; Verbal Fluency Tests; Design Fluency Tests; Color-Word Interference Test; Twenty Questions Test; and Tower Tests.
Design and Methods
IBM SPSS 23.0 was used to obtain descriptive statistics for the control and TBI groups. All analysis were based on a Cronbach’s alpha 0.05. The hypotheses were tested using appropriate independent-samples tests, which included t-tests for parametric data and a Mann-Whitney U for nonparametric analysis of data not meeting parametric assumptions to determine whether statistically significant differences existed in executive functioning performance between groups (bilingual and monolingual subjects) on the D-KEFS. Furthermore, age was treated as a continuous variable and was tested for normality.

Hypothesis 1
It is hypothesized that age would be a significant contributor to performance on executive functioning tasks among the TBI and control groups.
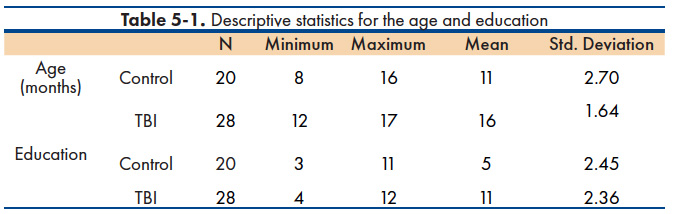
Descriptive statistics and results of the statistical tests are shown in Table 5-5. Age was treated as a continuous variable, and was tested for normality. It was found to be normally distributed for both TBI and control groups. The mean age for the TBI group was 192.3 months (SD = 18.3), and the median was 197 months. The mean age for the control group was 146.1 months (SD = 32.1), and the median was 144 months.
Regression analyses were used to fit models to each outcome variable, with age as a predictor, separately for TBI and control groups. The model-predicted values are plotted against the actual values for each outcome variable, with TBI and control groups presented together.
The models have reasonably good fits to the data. Even so, the R-squared values were relatively poor, with the highest value of 14.7% for Verbal – VF1. This is likely the result of having a smaller sample size. Results indicate that there were no statistically significant associations between the outcome variables and Age.
Hypothesis 2
It was hypothesized that neurocognitive performance on measures of executive functioning will be lower for the TBI group when compared to the control group. Results are compiled into Table 5-6.
Statistical comparisons of mean difference from the control group to those of the TBI group were made for each of the variables in Table 5-4. The results indicated a significant difference between groups for CW4 [t(36)=3.121, p =.003], TMT 2 [t(40)=3.175, p =.003], and TMT 3 [t(40)=3.259, p =.002]. In each instance, the mean difference between the control and TBI groups was 17 points or higher in the control group.


Hypothesis 3
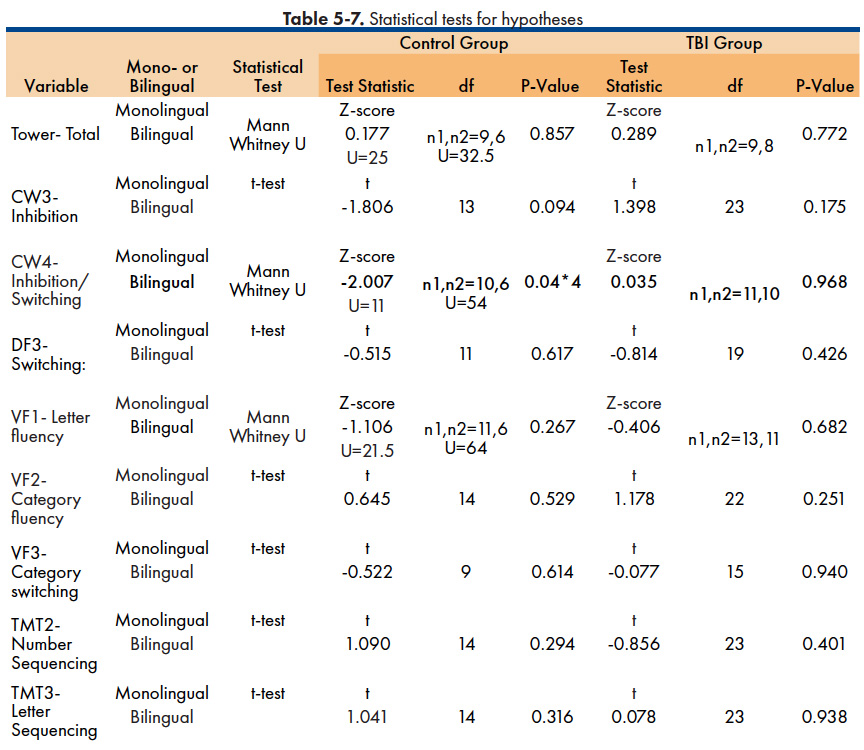
It was hypothesized that neurocognitive performance on measures of executive functioning will be lower for monolinguals as compared to bilingual peers. Descriptive statistics and results of the statistical tests are shown in Table 5-7.
Color Word 4 – Inhibition/Switching The data for this variable were tested for normality and found to be non-normally distributed. A Mann-Whitney U test was used to compare monolingual children to bilingual children. There were found to be statistically significant results for the control group (Mann Whitney U = 11, n1=10, n2=6, p=0.044), but not for the TBI group (Mann Whitney U = 54, n1=11, n2=10, p=0.968). This indicates that the Color Word 4 score representing inhibition/switching was affected by the TBI, such that mono- and bi-lingual children did not differ in the TBI group, whereas mono- and bi-lingual children significantly differed in the control group.
There were found to be no statistically significant results for the rest of the variables for either the control group or TBI group.

Based on the understood relationship between age and neurocognitive performance, it was hypothesized that age would be a significant contributor to executive functioning among the current TBI sample. Research has previously suggested that bilingualism promotes the integrity of white and grey matter in elderly individuals, increasing their cognitive reserve abilities (20, 21). However, due to the practice effect, the bilingual advantage has been found to be stronger in older adults as opposed to younger bilinguals. Contrary to what research suggests, this study did not generate significant results. A plausible explanation for these surprising results could be related to the older age of the participants of this study and the small sample size. Given these characteristics, the current finding might not be generalizable to the general population.
The main purpose of the current research investigation was to evaluate the difference between bilingual speakers and monolingual children who have sustained a TBI and their performance on two measures of executive functioning. It was hypothesized that neurocognitive performance on measures of executive functioning would be lower for the TBI group as compared to the control group. Supporting this hypothesis, results of the current study revealed that within the current population examined, there was a clinically significant difference in certain measures of executive functioning between patients with a TBI, as compared to those without a TBI. Explicitly, clinically significant differences were found in three verbal and non-verbal subtests of the DKEFS. The results of this study, demonstrated that the control group had higher scores as compared to the TBI group. Tavano, et al. (6) suggested that the frontal lobe’s higher order abilities seem to be a common cognitive sequel after a brain injury. Commensurate, this study found that the mean of a measure of verbal inhibition and switching was 17 points higher, while the mean of two tasks of non-verbal sequencing was 18 points higher. These results demonstrate children’s higher order functioning abilities were significantly impacted by a TBI. These results are consistent with previous research demonstrating that TBI is most likely to involve frontal and temporal brain areas which are the last to prune (7).
The current study was particularly interested in examining the impact of TBI on a bilingual versus a monolingual brain. For this reason, it was also hypothesized that neurocognitive performance on measures of executive functioning will be lower for monolinguals as compared to bilingual peers. Partially supporting hypothesis III, this study found a clinically significant difference in the control group, in which bilingual children outperformed monolinguals in the scores for the DKEFS Color Word 4 – Inhibition/Switching, a measure of verbal executive functioning. The Color Word 4 task is believed to be a measure of both mental flexibility and the ability to inhibit a dominant response. Researchers propose this is a skill that bilinguals actively practice when switching/inhibiting a second language (16, 17).
Not surprisingly, the Stroop Task, which is similar to the DKEFS Color Word 4 – Inhibition/Switching subtest of the DKEFS, have been used multiple times in research to compare executive functioning of monolinguals versus bilinguals.
Wang, et. al. (23) explains:
Stroop effect is a combined result of cognitive control and word recognition suggests that the reduction of the Stroop effect in bilinguals is caused not only by their enhanced cognitive control (Bialystok et al., 2008), but also by their delayed word recognition. Bilinguals enjoy better cognitive control than monolinguals, which helps to better inhibit the interference of the irrelevant lexical semantic information from the printed word and in turn to reduce the Stroop interference. In addition, as bilinguals have slower word recognition than monolinguals due to their reduced frequency of use in either of their languages (e.g., Gollan et al., 2008), the recognition of the irrelevant word should be delayed, leading to a further reduction of the Stroop effect. (p. 99)
Bialystok (16) concluded that the most consistent finding about the neurocognitive advantage of bilingual children is the favorable selective attention and inhibition. Putting this evidence together, might explain why bilinguals outperformed monolinguals in a verbal task of inhibition and switching and why that advantage was not seen in other non-verbal measures that are commonly used, such as the DKEFS Trails and Tower. Trails test is a measure of switching rather than inhibition. Also, it does not have a verbal component, on the other hand, the Tower test measures organization and planning. These findings suggest that Color Word 4 is the measure that best captures the bilingual advantage, as it includes inhibition of irrelevant information, as well as it requires word recognition. This finding has important implication for neuropsychological work with bilingual populations. The results of this study implicate that the DKEFS Color Word 4 – Inhibition/Switching subtest should be included in neuropsychological batteries used with bilinguals.
This study did not find significant differences in any of the verbal measures of executive functioning. Previous research has shown that bilinguals have slower responding and that the verbal abilities of bilinguals are deficient in both languages when compared to monolinguals (24). Lauchlan (25) found that the effortful steps required for word searching among a massive vocabulary bank (accumulative vocabulary of the two languages) might explain stammering, as inhibitory control is not fully developed in the early stages of language development, which in the current study, was expected to impact the performance of bilingual children in the Verbal Fluency subtests as measured by the DKEFS.
A significant finding from the current study was the lack of evidence to support that bilingualism acts as a protective factor after a TBI. These results suggest that bilingual children without a TBI history may benefit from being bilinguals, whereas that advantage was not found for bilingual children after sustaining a TBI. Research has found that cognitive sequels of a TBI are correlated with the current developmental stage. The results of this study might be explained by the development of the brain. The frontal lobe, the part of the brain responsible for higher-order cognitions, is not fully developed in children. Thus, after sustaining a TBI the frontal lobe might fail to undergo the expected pruning and myelination (7). Pruning is characterized by the loss of grey matter volume, which in turn, is correlated with the development of complex cognitive abilities, such as executive control (7). Previous research and this current study concur in that damage to less mature regions of the brain (such as the frontal lobe) is likely to produce life long difficulties in cognitive functions and emotional control (7), that counteracts with the bilingual advantage observed in the control group. As opposed to children, bilingual adults have been found to able to endure higher brain damage before cognitive functioning impairment, as opposed to those with lower cognitive reserve (monolinguals) (20). Other than brain development, this contrast might also be related to adults having the opportunity to practice being bilinguals for a longer time. Luo, L., Luk, G. & Bialystok, E. (26) suggested that longer duration of bilingualism is associated with the bilingual advantage.
In conclusion, bilinguals without a TBI demonstrated a significant advantage in a verbal task of inhibition and switching. Overall results demonstrate children’s higher order functioning abilities are significantly impacted by a TBI. Interestingly, bilingual children seem to be at an increased risk of executive functioning impairments after a TBI. This could be the result of a newly acquired skill and the damage to a less mature region of the brain. For this reason, bilingual children who are in the process of acquiring a new skill (a second language), might fail to benefit from the “advantage” of being bilingual if they sustain a TBI and may have more deficits when compared to monolingual children.
In general, the TBI group had older subjects, which contrary to what it is suggested, should demonstrate improved executive functioning abilities. However, a very important factor that was not possible to be analyzed with this sample is the age of injury, which was not available in the archival data. One of the most salient limitations to the current study was the sample size. As only 48 children were included in this study, a larger sample size would increase the power to the statistical analysis. Another limitation of the study was that the population examined was a clinical sample. Although certain measures were put in place, such as including a control group, results obtained may not generalize to a non-clinical population. Additionally, there was a variety of conditions/diagnoses within the disorders included in the sample, due to the overall characteristics of the clinical group. Research has found that certain disorders, such as ADHD, have an impact on the performance of executive functioning measures. In this study, certain subjects in the TBI group had a diagnosis of ADHD, which was used as an exclusion criterion for subjects in the control group. Even though the control group that was included was meant to help understand the difference between monolingual and bilingual children with and without a TBI, given the clinical characteristics of this sample and the differences in demographics (e.g. educational level, age), it is believed to be a weakness of this present study and not a good representation of these differences.
Additionally, the bilingual group was considered to be heterogeneous as some subjects spoke more than two languages. Although it was not possible in this study due to the small sample size, it would be interesting to divide the groups by monolingual, bilingual, and multilingual. Moreover, proficiency level was not taken into consideration for the current study. This limitation was based on available measures to assess for language proficiency. Although some subject did complete the Woodcock Johnson Oral Language, not all subjects included in this study had completed the measure. It is well known that language proficiency, that which is self reported and that is reported by parents, might be inaccurate during neuropsychological evaluations. However, to the best of the licensed clinical neuropsychologist knowledge, reported language proficiency was accurate.
The inconsistent results found could be further investigated by controlling for the age of injury. It is well known that young brains might be vulnerable to more severe and enduring deficits as new abilities are emerging. Additionally, skills established at one stage form the foundation for later-developing abilities. Based on this, if a child has a brain injury at a younger age, the higher order cognitions might not developed to its fullest, as opposed to a brain injury at a later stage of development. Since this study is among the first to examine executive functioning in a monolingual and bilingual clinical population, future research should examine a larger sample size and attempt to compare bilinguals versus multilingual with both clinical and non-clinical populations. It would be extremely valuable in the future to compare the executive functioning performance between balanced versus unbalanced bilinguals, as well as explore the differences and similarities between the languages spoken by the sample. Careful consideration should be taken when considering the clinical implications of these results, as the performance on standardized tests differs between Caucasians and individuals from other ethnicities.
- Delis, D. C., Kaplan, E., & Kramer, J. H. Delis-Kaplan executive function system. San Antonio, TX: The Psychological Corporation; 2001.
- Tatla, S. K., Sauve, K., Jarus, T., Virji-Babul, N., & Holsti, L. The effects of motivating interventions on rehabilitation outcomes in children and youth with acquired brain injuries: A systematic review. Brain Injury. 2014; 28(8), 1022-1035.
- Pomerleau, G., Hurteau, A., Parent, L., Doucet, K., Corbin-Berrigan, L., & Gagnon, I. Developmental trajectories of infants and toddlers with good initial presentation following moderate or severe traumatic brain injury: A pilot clinical assessment project. Journal Of Pediatric Rehabilitation Medicine. 2012; 5(2), 89.
- Soo, C., Tate, R., & Brookes, N. Psychosocial adjustment following acquired brain injury in childhood and adolescence: Executive, behavioural and emotional contributions. Brain Injury. 2014; 28(7), 906-914.
- Tavano, A., Galbiati, S., Recla, M., Bardoni, A., Dominici, C., Pastore, V., & Strazzer, S. Cognitive recovery after severe traumatic brain injury in children/adolescents and adults: Similar positive outcome but different underlying pathways? Brain Injury. 2014; 28(7), 900-905.
- Tavano, A., Galbiati, S., Recla, M., Formica, F., Giordano, F., Genitori, L., & Strazzer, S. Language and cognition in a bilingual child after traumatic brain injury in infancy: Long-term plasticity and vulnerability. Brain Injury. 2009; 23(2), 167-171.
- Wilde, E. A., Hunter, & Bigler, E. D. Pediatric traumatic brain injury: Neuroimaging and neurorehabilitation outcome. Neurorehabilitation. 2012; 31(3), 245-260.
- Brown, F. L., Whittingham, K., Boyd, R. N., McKinlay, L., & Sofronoff, K. Improving child and parenting outcomes following paediatric acquired brain injury: a randomised controlled trial of Stepping Stones Triple P plus Acceptance and Commitment Therapy. Journal Of Child Psychology & Psychiatry. 2014; 55(10), 1172-1183.
- Egede, L. E., Dismuke, C., & Echols, C. Racial/Ethnic Disparities in Mortality Risk Among US Veterans With Traumatic Brain Injury. American Journal Of Public Health. 2012; 102(2), 266-271.
- Grosjean, F. Neurolinguists, beware! The bilingual is not two monolinguals in one person. Brain and Language. 1989; 36, 3–15.
- Girbau, D., & Schwartz, R. G. Phonological working memory in Spanish-English bilingual children with and without specific language impairment. Journal of Communication Disorders. 2008; 41, 124–145.
- Calabria, M., Marne, P., Romero-Pinel, L., Juncadella, M., & Costa, A. Losing control of your languages: A case study. Cognitive Neuropsychology. 2014; 31(3), 266-286.
- Banich, M. T. Executive function. In C. Hartford (Ed.), Cognitive neuroscience and neuropsychology. Boston, MA: Houghton Mifflin; 2004. p. 365–392
- Calvo, A. & Bialystok, E. Independent effects of bilingualism and socioeconomic status on language ability and executive functioning. Cognition, 2014; (3) 278-288.
- Bialystok, E. Global–local and trail-making tasks by monolingual and bilingual children: beyond inhibition. Developmental Psychology. 2010; (1) 93.
- Bialystok, E. Reshaping the mind: the benefits of bilingualism. Canadian Journal Of Experimental Psychology. 2011; (4) 229.
- Bialystok, E., Craik, F. I., & Luk, G. Review: Bilingualism: Consequences for mind and brain. Trends In Cognitive Sciences. 2012; (16) 240-250.
- Bialystok, E., Craik, F., & Luk, G. Cognitive control and lexical access in younger and older bilinguals. Journal Of Experimental Psychology: Learning, Memory, And Cognition. 2008; 34(4), 859-873.
- Miyake, A., Freidman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognitive Psychology. 2000; 41, 49–100.
- Guzmán-Vélez, E., & Tranel, D. Does bilingualism contribute to cognitive reserve? Cognitive and neural perspectives. 2015; 29(1), 139-150.
- Costa, A., & Sebastian-Galles, N. How does the bilingual experience sculpt the brain?. Nature Reviews Neuroscience. 2014; (5) 336.
- Friedman, N. P. Research on individual differences in executive functions. Linguistic Approaches To Bilingualism. 2006; 6(5), 535-548.
- Wang, R., Fan, X., Liu, C., & Cai, Z. G. Cognitive control and word recognition speed influence the Stroop effect in bilinguals. International Journal Of Psychology. 2016; 51(2), 93-101.
- Poulin-Dubois, D., Bialystok, E., Blaye, A., Polonia, A., & Yott, J. Lexical access and vocabulary development in very young bilinguals. International Journal Of Bilingualism. 2013; 1, 57-70.
- Lauchlan, F. The nature of bilingualism and implications for educational psychologists. Educational & Child Psychology. 2014; 31(2), 8-20.
- Luo, L., Luk, G. & Bialystok, E. Effect of language proficiency and executive control on verbal fluency performance in bilinguals. Cognition. 2010; 1, 29–41.

